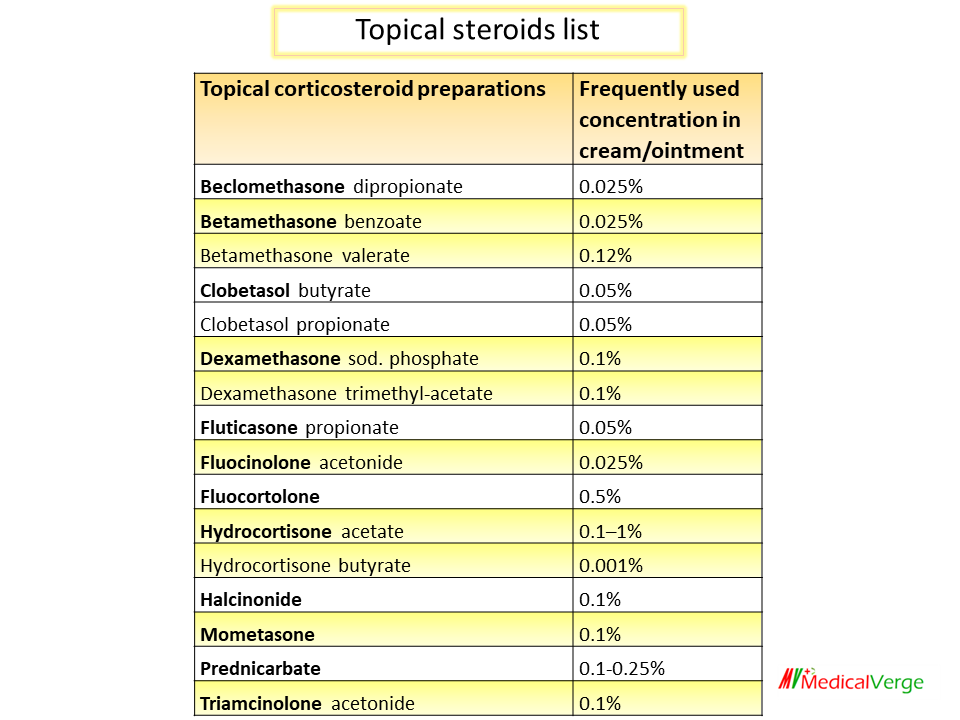
Topical steroids are used to treat a wide range of dermatological illnesses. Their anti-inflammatory, immunosuppressive, vasoconstrictor, and antiproliferative (for scaling lesions) properties are major mechanism to use them topically. The extent of absorption to deeper layers determines the strength of action, and hence the lipophilicity of the molecule determines potency to a large extent. Fluorinated or lipid-soluble esters of glucocorticoids are effective topically, e.g., hydrocortisone butyrate. Topical steroid preparations include the following:
Topical steroids list
Topical corticosteroid preparations
Frequently used concentration in cream/ointment
Beclomethasone dipropionate
0.025%
Betamethasone benzoate
0.025%
Betamethasone valerate
0.12%
Clobetasol butyrate
0.05%
Clobetasol propionate
0.05%
Dexamethasone sod. phosphate
0.1%
Dexamethasone trimethyl-acetate
0.1%
Fluticasone propionate
0.05%
Fluocinolone acetonide
0.025%
Fluocortolone
0.5%
Hydrocortisone acetate
0.1–1%
Hydrocortisone butyrate
0.001%
Halcinonide
0.1%
Mometasone
0.1%
Prednicarbate
0.1-0.25%
Triamcinolone acetonide
0.1%
topical steroid list
General guidelines for steroidsuse topically
The steroid’s penetration varies considerably depending on the site: high in the face, scalp, axilla, groin and scrotum; medium in the limbs and trunk; and low in the palm, sole, elbow and knee. Potent preparations should be avoided in areas with high penetration because they are prone to side effects. Milder agents are usually ineffective in areas with low penetration.
Absorption into the skin is also affected by the nature of lesion: atopic and exfoliative dermatitis have high absorption, while hyperkeratinized and plaque-forming lesions have low absorption. Acute lesions should be treated with milder drugs, whereas chronic lesions should be treated with stronger ones.
It’s crucial to pick the right vehicle. Exudative lesions respond better to lotions and creams, which allow for evaporation and have a cooling, drying, and antipruritic action. For hairy areas, sprays and gels are suitable. Ointments are reliable for chronic, scaly lesions because they generate an occlusive coating.
Occlusive dressing promotes bacterial and fungal growth. Continuous occlusion increases steroid absorption by up to tenfold, preserves moisture, and causes maceration of the horny layer. Intermittent occlusion of chronic, hypertrophied lesions is acceptable (12 hours at a time).
The usage of potent steroids on a routine basis is not justified. Highly potent preparations should be used only for severe inflammatory disorders, such as unresponsive eczema, psoriasis, and only for a short duration until the lesion heals. It is best to apply the mildest preparation that will control the lesion.
Potent preparations should be use for short duration or intermittently to avoid adverse effects and tolerance. Sudden discontinuation should be avoided. If the condition improves, a less strong preparation can be used instead, or the steroid can be replaced with an emollient until the lesion heals. Skin of face is more susceptible, hence potent halogenated steroids not to be used on face.
In infants and young children, absorption is greater, thus milder drugs should be applied.